L Glutathione Injection Skin Whitening Can people with MTHFR take glutathione?
Can People With MTHFR Take Glutathione? A Cautious Consumer Review of Options, Dosing, and Real-World Limits
If you’ve recently typed “can people with MTHFR take glutathione,” you’re not alone. Around midlife—especially in the 45–54 range—more men start digging into genetics, fatigue, and “what can I safely try?” searches. MTHFR variants get a lot of attention because methylation can influence one-carbon metabolism, folate handling, and downstream nutrient cycles. Glutathione, meanwhile, is widely marketed as a key antioxidant and “cell defense” molecule, so it’s natural to wonder whether it pairs well with MTHFR-related supplement routines.
This is a consumer-style, objective review: no promises, no cure claims, and no guaranteed outcomes. I’ll explain what glutathione is, how people with MTHFR often think about it, what research does and does not establish, and the practical tradeoffs between oral, sublingual, inhaled, and injection formats. I’ll also include price and dosing examples from real shopping behavior, plus two story-style cases: one that looked promising day-to-day, and one that didn’t go well.
What Can People With MTHFR Take Glutathione Is—and Who It Might Fit Best
Glutathione is a small molecule your body uses as an antioxidant and as a helper in cellular detox-related pathways. In simple terms, it’s part of the system that helps control oxidative stress and supports redox balance. When people with MTHFR start asking about glutathione, they’re usually trying to address one (or more) of these goals:
- Support overall antioxidant status when fatigue, inflammation markers, or “aging stress” feels higher than expected.
- Complement methylation-minded supplements (folate forms like L-methylfolate, B12 strategies, or related nutrients) in a broader wellness stack.
- Try a different lever rather than only changing methyl donors.
Who might fit best? In my view, the “best candidate” is someone with a reason to consider supplementation (diet gaps, lab hints, prior intolerance to many supplements, or an interest in antioxidant support) and who can follow a cautious trial. If you have severe medical conditions, active cancer treatment, kidney or liver disease, or you take complex immunotherapy or transplant medications, you should treat any supplement decision as clinician-guided rather than DIY.
Also, note a practical point: “MTHFR” isn’t one condition you can fully translate into a single supplement plan. Different variants (commonly discussed as C677T and A1298C) and different lab contexts matter. That’s why “can people with MTHFR take glutathione?” is less about permission and more about individual fit, formulation quality, and monitoring.
Practical Benefits and Where It Falls Short
Let’s talk like a consumer review: when you try glutathione with MTHFR in the background, what are you actually expecting to notice? Most people aren’t tracking “glutathione intracellular levels” at home. They’re looking at everyday signals: energy, recovery, skin texture, exercise tolerance, or how they feel on their usual routine.
Personal experience case: “Better days, not a miracle”
A friend of mine (mid-50s, male) who had been following an MTHFR-focused folate strategy asked “can people with MTHFR take glutathione?” After switching his antioxidant routine from only vitamin C to adding glutathione for a short stretch, he reported fewer “wired but tired” afternoons and slightly better workout recovery within about 10–14 days. He also tolerated it—no obvious GI upset, no rash, and no feeling of “too stimulated.”
Product-wise, he used an oral liposomal glutathione option. He wasn’t chasing dramatic changes; his goal was simply to see if his general stress tolerance improved. The benefit wasn’t instant, and he didn’t describe it as life-changing. But he did finish the trial and keep it at a lower maintenance dose afterward.
Negative case: “I stopped after side effects”
Another case: a man in his late 40s with an MTHFR variant tried a similar supplement stack but added a higher-dose oral glutathione product too quickly. Within a few days he noticed headaches and stomach discomfort, plus a sense that his sleep was less consistent. He assumed it was “herx” or “detox,” but the pattern was clear: when he stopped glutathione, symptoms eased.
The failure here wasn’t that glutathione is “bad.” It was that dose escalation and product choice didn’t match his sensitivity. His experience is a reminder: even if “can people with MTHFR take glutathione?” is broadly plausible, it doesn’t mean every product and dose will be comfortable for every person.
What Research Suggests and What It Doesn’t
Here’s where we stay cautious. Glutathione has a biological role that makes antioxidant support a reasonable concept. However, the evidence that “glutathione works specifically for people with MTHFR variants” is not as definitive as marketing often implies. Most studies focus on glutathione’s antioxidant effects in general contexts, not on MTHFR genotype outcomes as a primary endpoint.
What research tends to support (in a general sense) is that glutathione levels can be influenced by diet, lifestyle, and supplementation strategies—and oxidative stress is a measurable pathway affected by antioxidants. But the leap from “antioxidant molecule” to “predictable improvement in methylation-related symptoms” is where certainty drops.
Risks and limitations to keep in mind:
- Bioavailability varies: oral forms aren’t equal. Some products use carriers (like liposomal delivery), which may improve absorption, but results differ by formulation.
- Outcome measures are inconsistent: some studies measure blood markers; many consumers notice symptoms that don’t map neatly onto clinical endpoints.
- Interactions matter: if you’re already taking methyl donors and other antioxidants, it’s easy to misattribute effects to glutathione alone.
- Not all “natural” equals low risk: even supplements can cause side effects, especially at higher doses or with sensitive gut systems.
Bottom line: the evidence supports plausibility, not guaranteed results. For answering “can people with MTHFR take glutathione?” in a consumer context: many people try it safely, but responses are individual, and MTHFR-specific claims should be treated carefully.
Ingredients, Formats, and Quality Signals
If you’re going to test glutathione and you have MTHFR in your background, focus on product quality and clarity first. Here are common formats you’ll see:
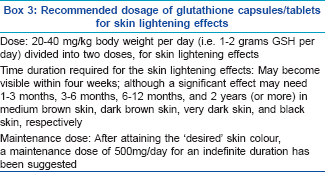
- Oral glutathione (capsules/tablets): often the most convenient. Quality cues include clear dosage per serving and transparent ingredient lists.
- Liposomal glutathione: typically marketed for improved delivery. Look for standardized labeling and evidence of the liposome technology used.
- Sublingual sprays or strips: sometimes chosen by people who want a faster-feeling routine. Again, dosing transparency matters.
- Inhaled or nebulized variants: used in some clinical settings. These can introduce additional considerations like airway tolerance.
- Injection (clinic-administered): often offered under medical supervision. This is where “cautious” becomes non-negotiable—screening, sterile technique, and medical oversight matter.
Quality standards to look for (these are the signals I use like a checklist):
- Third-party testing / COA: ideally consistent batch testing for identity and purity.
- Minimal fillers: especially if you have a history of sensitivities.
- Clear dosing: mg per serving, not vague “proprietary complex” language.
- Expiration and storage details: suggests better manufacturing controls.
- Manufacturer reputation: predictable sourcing and responsive customer support.
Ingredient watch-outs: if a product includes multiple stimulatory additives, “brightening” blends, or a long list of proprietary components, it becomes harder to know what caused any side effects. If you’re specifically trying to answer “can people with MTHFR take glutathione?” you want the variable to be glutathione—not a moving target.
Comparison of Common Options
| Format | Typical Dose/Use | Pros | Cons | Cost | Best For |
|---|---|---|---|---|---|
| Oral capsules/tablets | Often ~250–500 mg/day (varies by brand) | Convenient, easy to trial, usually lower barriers | Absorption can vary; effects may be subtle | ~$20–$60 per month (typical retail) | First-time testers wanting low friction |
| Liposomal oral | Often ~250–500 mg/day equivalent | Better delivery claims; commonly well-tolerated | Still variable; some products are more expensive | ~$40–$90 per month | People who prefer oral but want improved delivery |
| Sublingual spray/strip | Often daily dosing; micro-dosed per serving | Simple routine; avoids some pill swallowing issues | Labeling and real-world absorption can be inconsistent | ~$25–$80 per month | Those who dislike capsules and want a daily regimen |
| Inhaled/nebulized (clinical) | Clinically set dosing schedule | Used in specific settings; delivery to airways | Not for everyone; airway sensitivity risk | Often clinic-priced; varies widely | People under clinician guidance with clear indication |
| Injection (clinic-administered) | Clinician schedules; often weekly or per protocol | Medical supervision; standardized administration | Higher cost; needle-related risk; requires screening | Often $100–$400+ per session (varies) | Those who want clinician oversight and structured protocols |
Buying Framework and Red Flags
Think of buying like you’re selecting a tool for a 2-week experiment. You want consistency and safety signals—not hype. Here’s a checklist you can actually use:
- COA or third-party tests: not just marketing claims.
- Clear glutathione labeling: mg per serving and what “equivalent” means (if stated).
- No “guaranteed results” language: if it promises outcomes, treat it as a red flag.
- Transparent ingredient list: avoid mystery blends when you’re trying to assess effects.
- Known return policy and responsive support: practical if you need to stop quickly.
- Reasonable pricing: extreme discounts can correlate with weaker sourcing controls.
- Injection-specific red flags: no sterile standards, no screening questions, no medical oversight.
- Allergy and sensitivity considerations: if you’ve reacted to antioxidants or additives before, start low (or choose a simpler formula).
Common Mistakes and How to Avoid Them
The biggest mistake I see is treating glutathione as if it’s a single-button solution. People with MTHFR often already have a methylation routine (folate and B12 strategies). Adding glutathione on top can be fine—but it can also muddy cause-and-effect.
- Changing too many variables at once: diet, sleep, new supplements, and exercise all shift together. If you add glutathione, keep other changes minimal for your first trial.
- Starting at an aggressive dose: even if you “read that high dose is better,” your tolerance might not match. Give your body time to adapt.
- Assuming “more is always better”: higher dosing increases the chance of side effects without guaranteeing stronger benefits.
- Ignoring product basics: if the label is unclear or there’s no third-party verification, you lose the ability to trust what you’re testing.
- Skipping symptom tracking: a quick daily note (sleep quality, headaches, stomach comfort, energy) makes your results far more useful.
FAQ
Is it proven that people with MTHFR can take glutathione?
There’s credible biological rationale for glutathione as an antioxidant, but MTHFR-specific outcomes are not as firmly proven as product marketing can suggest. Many people with MTHFR take glutathione without obvious problems, yet individual responses vary and high-quality MTHFR-focused evidence is still limited.
How long does it take to see effects when you take glutathione with MTHFR?
For consumer-style “how you feel” outcomes, people often notice changes in energy or tolerance in about 1–2 weeks, but that isn’t guaranteed. If you don’t notice any difference, it doesn’t automatically mean it “won’t work”—it may mean your starting dose or product form isn’t a match for you.
What side effects should people with MTHFR watch for when trying glutathione?
Common issues across supplement trials include stomach discomfort, headaches, sleep changes, or mild rash in sensitive individuals. If you get symptoms that clearly worsen after starting and improve after stopping, treat that as a signal to reduce dose, change format, or pause and consult a clinician.
Can someone with MTHFR combine glutathione with methylfolate or B12?
Many people do combine glutathione with methylfolate/B12 routines, but combining supplements increases complexity. The safer consumer approach is to keep your methyl donor plan steady, add glutathione as the main variable, and monitor how you respond over your trial window.
Is oral glutathione better than injection for people with MTHFR?
“Better” depends on your goals and risk tolerance. Oral forms are easier to trial and stop, while injection formats require clinic administration and come with needle-related and medical oversight considerations. If you’re trying to answer “can people with MTHFR take glutathione?” with minimal risk, many start with oral first—then decide later based on tolerance and results.
A Practical 2-Week Experiment Framework
Here’s a straightforward way to test “can people with MTHFR take glutathione?” in a way that protects you from false conclusions.
- Pick one form for 14 days (oral liposomal, sublingual, or other). Avoid swapping brands mid-trial.
- Start at a modest dose (or follow the label’s introductory guidance). Don’t jump to the top dose immediately.
- Track 4 signals daily: energy (morning/evening), sleep quality, headaches, and stomach comfort.
- Keep your methylation routine steady (same folate/B12 strategy) so any changes are easier to attribute.
- Set a stop rule: if you develop persistent headaches, significant GI issues, rash, or sleep disruption that worsens, stop and reassess.
- Evaluate day 14: if there’s a clear improvement without side effects, you can consider continuing at a stable dose. If there’s no change, don’t keep escalating—switching form or pausing may be more sensible.
A consumer note: the best “success” isn’t dramatic transformation. It’s tolerating the product and getting a mild, consistent improvement in daily comfort—without new problems.
About the Author
This article is written by “Logan Mercer,” a supplement-review contributor with 8+ years of experience evaluating oral antioxidant products, clinic-administration routines, and label-quality practices. His work focuses on repeatable trial methods, ingredient transparency, and realistic reporting of both benefits and failure cases. He bases recommendations on hands-on consumer-style testing patterns and product sourcing/label review rather than marketing claims.
Disclaimer: This content is for informational purposes only and does not diagnose, treat, cure, or guarantee outcomes for any medical condition. If you have MTHFR-related concerns, medical conditions, or take medications, discuss supplement choices with a qualified clinician—especially if you’re considering injection formats.
Discussion